January 23, 2023
Abstract
The COVID-19 pandemic has illuminated the stark inequities between the Global North and Global South in vaccine production and access. Such inequities are a continuation of asymmetrical power relations rooted in historical racialized processes such as slavery and colonialism and its post-colonial legacies which led to the subordination of many countries in the Global South. This paper connects global vaccine inequity with the concept of racial capitalism, the latter being a concept which refers to processes of deriving economic value from the racial identity of another person. Racial capitalism allows us to frame our understanding of the dynamics underlying vaccine inequities as colonial legacies imbued with racial capitalist logics and highlight why many of the solutions offered to address these inequities are likely to manufacture inequality in future crises. This paper begins by providing a brief account of racial capitalism’s relationship to global vaccine inequity. What then follows is an analysis of the role of global health law in creating and sustaining imperial extractive relationships that disadvantage countries in the Global South and engender vaccine inequity. This analysis helps to illuminate the racially-capitalist nature of some of the potential “solutions” to COVID-19 vaccine inequity, such as COVAX and C-TAP, which are then critiqued. The final sections then explore new initiatives to scale-up vaccine manufacturing in the Global South which seek to redress inequities, as well as the role that reparative justice (reparations for historical injustices) could play in creating more equitable pathways to vaccine equity through reforming international intellectual property law and creating new financing arrangements for supporting vaccine manufacturing in low- and middle-income countries.
Introduction
Colonial legacies, racial capitalism, and vaccine inequity
In the wake of the COVID-19 crisis, the U.N. Secretary General António Guterres recently argued that racism is a catalyst of global inequality[1]. He urged countries to collectively recognize and attempt to reverse historical injustices that continue to reverberate today, including “the lingering traumas, the suffering across generations, the structural inequalities so deeply rooted in centuries of enslavement and colonial exploitation” through reparative justice frameworks[2]. While the history of the term “racial capitalism” is uncertain, it has been used by scholars for over forty years as a framework for viewing the mutually constitutive relationships of racialized and imperial exploitation within the process of capitalist accumulation. In the 1970s, South African Marxists and anti-apartheid activists were using racial capitalism to critique the political economy of white supremacy and capitalism[3]. North American scholars such as W.E.B. Du Bois, C.L.R. James, and Eric Williams also made correlations between racial capitalism and the introduction of industrial capitalism, slavery and colonialism. Cedric Robinson took the concept of racial capitalism further by first tracing the history of a racial hierarchy grounded in slavery which favors “whiteness”, arguing that capitalism was firmly rooted in the exploitation of race-based labor during Pre-modern slavery in Europe which continued during the era of colonialism[4]. While capitalism and racism both have their own distinct histories, it is clear that racial ideology was used as a way to oppress non-white populations in the quest to accumulate wealth by white populations[5].
Like other modes of capital accumulation, racial capitalism focuses on profit making through exploitation but there is a historical focus on the racial social stratification and its usefulness in re-examining colonial and post-colonial forms of extraction[6]. Racial capitalism has been used to understand other social and political processes such as settler colonialism in Palestine and South Africa[7], environmental and climate justice[8], contemporary international law on slavery[9], and also in understanding the persistence of racial inequities in formerly segregated countries such as the U.K. and U.S[10]. This paper builds on racial capitalism scholarship within studies of the COVID-19 crisis which critiqued the disproportionate mortality within populations[11] and unequal labor relationships[12], presenting a novel contribution by thinking through the systemic impacts of racial capitalism on the production of essential medicines, and particularly COVID-19 vaccines, in global health.
A deeper understanding of the systemic injustice in the international patent system enables us to center the experiences of the Global South through a re-examination of how international law sustains and encourages the geographic and racial stratification of vaccine manufacturing, which is now largely centralized in the Global North. Furthermore, framing our analysis through the lens of racial capitalism enables us to better understand why solutions offered to address inequalities of access to vaccines such as COVAX and the COVID-19 Technology Access Pool (C-TAP) not only failed to succeed but also merely serve to reinforce these racialized global inequalities.
In the following section, an analysis of the role of global health law in creating and sustaining imperial extractive relationships that disadvantage countries in the Global South and engender vaccine inequity help to illuminate the racially-capitalist nature of some of the potential “solutions” to COVID-19 vaccine inequity, such as COVAX and C-TAP, which are then subsequently critiqued. This paper then critiques new initiatives to scale-up vaccine manufacturing in the Global South that seek to redress inequities by arguing that a lack of attention to the underlying racially capitalist logics underlying these schemes threatens the viability of these initiatives. The final section offers two propositions for a global reparative justice agenda for vaccine equity, related to reforming the international intellectual property (IP) system and establishing long-term financing mechanisms to increase vaccine manufacturing capacity in the Global South.
How global health law was borne of and sustains racial capitalism
The ways in which existing geographies of power contribute to global health inequality has been a recurring theme in addressing COVID-19 vaccine inequity. International institutional settings and international legal frameworks which have histories rooted in colonial practice cannot produce equal outcomes for populations globally. Indeed, these frameworks have been shown to reproduce forms of colonial racialized violence[13]. In order to demonstrate the ways in which global health law was borne of and sustains racial capitalism, the first two subsections below consider the history of global health law, which is rooted in colonial medicine, and the ways in which it reemphasizes border enforcement as a mechanism of disease containment. The final subsection in this part analyzes the racial-capitalist logics in the internationalization of health, trade and intellectual property protection before going on to illustrate how these developments have compounded the historic geographical and racialized inequities in vaccine manufacturing.
The racialized nature of colonial medicine and the birth of international and global health law
The term “colonial medicine” refers to the ways in which health and medicine were used to protect the economic interests of colonizing powers. During the colonial era, the health of imperial agents and colonized subjects were perceived as necessary for the continued development of the colonial project[14]. Ill-health threatened economic enterprises through loss of productivity. Colonial medicine focused on treating “tropical” or “foreign” diseases, and it was not deemed necessary, practical or cost effective by colonial authorities to address the underlying social and economic determinants of illness in colonized territories[15]. After World War II, health decision making was relocated from colonial governments to new centers of international health based in the Global North, which ensured the continued hegemony of Western biomedicine[16]. Law played an integral role in maintaining racialized capitalist logics both materially and discursively. Firstly, when states gained independence, law was used by former colonial powers in the Global North to subordinate post-colonial states through implementing treaties which curbed the latter’s sovereignty[17]. Secondly, and more successfully, law was used to promote the interests of corporations, which are vehicles for the racialized creation of state wealth[18]. Economic exploitation and expansion for profit was historically aided by corporations acting on behalf of colonial governments who granted them trading monopolies[19]. Neo-colonial legacies still shape capitalist aspirations in the ways in which post-colonial states provide extraction grounds for former colonial powers. The social construction of “race” was used to legitimize post-colonial expansion through the signing of international treaties which continued to consolidate power in the Global North. These unequal power dynamics manifested in global access to medicines arrangements through the reorganization of intellectual property rules from the World Intellectual Property Organization (WIPO) to the World Trade Organization (WTO). WIPO was more egalitarian in nature and focused on the public good, however, as international patent rights became governed and enforceable though the WTO’s Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPS Agreement), this new configuration became more concerned with protecting the interests of large corporations which prevailed over notions of the public good.
Racialization in health-related border enforcement practices
The expansion of European operations in the Global South led to the transmission of new infectious diseases, for which indigenous populations had no immunity, decimating the populations of colonized nations. Despite this, pandemics and the spread of infectious diseases have historically led to the racialization of border enforcement, with countries in the Global South being historically perceived as vectors of disease. The history of law making in global health illustrates this point. Between 1851 to 1938, fourteen international sanitary conferences attempted to prevent infectious diseases from making their way to Europe and North America. In instances where entry into Europe and North America by former colonial subjects was permitted, many countries were subjected to stringent quarantine rules, especially for cholera, typhus and yellow fever, which were all perceived as “foreign” health threats. By the 21st century, only vaccines for yellow fever would remain an entry requirement for countries in the Global North, but the requirement to be vaccinated fell primarily on people from the Global South[20]. Similarly, during the COVID-19 crisis, we saw how borders were simultaneously used to keep citizens of the Global South out of countries of the Global North unless they were “desirable” migrants needed to fill employment shortages in some industries, while giants such as Amazon were given unobstructed access to deliver consumer goods across borders[21].
The internationalization of trade and intellectual property
International IP rights, whether adopted in accordance with the Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPS), or subsequent bilateral and multilateral agreements, are part of a wider legal system which facilitates racial capitalism globally. Modern IP rights are derived from property rights that have a longer history rooted in John Locke’s labor theory of private property which was central to colonial aspirations from the 17th century[22]. Over time, the definition of property was expanded to include IP, which has had a significant impact on access to medicines, owing to the patenting of life saving medications. As Amaka Vanni argues, “a historical examination of the contemporary patent regime shows how colonialism, racism, and inequality became deeply sedimented into the international IP law, particularly patents, to enforce a particular type of property rights and to protect the economic interest of the transnational capitalist class”[23].
Global South nations have also been forced to accept more stringent patent protections to gain trade advantages and to avoid trade sanctions when these bilateral and multilateral agreements are entered into[24]. This largely benefits pharmaceutical corporations who are domiciled in the Global North because international IP law both facilitates the commodification of medicines that are essential to human survival and wellbeing for racialized people in the Global South and sacrifices the lives and health of the poor and otherwise marginalized on the altar of corporate profitability.
The COVID-19 pandemic has forced us to re-examine how international IP law impedes equitable global access to essential medicines and leads to drug shortages and increased prices in ways that disproportionately impact on Global South populations. By early December 2022, many countries in the Global North had vaccinated at least 80 percent of their populations, while many countries in the Global South had not even achieved 25 percent of vaccination rates (see Fig. 1). This stark inequality was labelled by activists as “vaccine apartheid”, a powerful term which highlights the elements of imperialistic structural violence underpinning it[25]. We can therefore see vaccine inequity as a continuation of racist double standards and exclusions from the age of empire into the neo-colonial present[26].
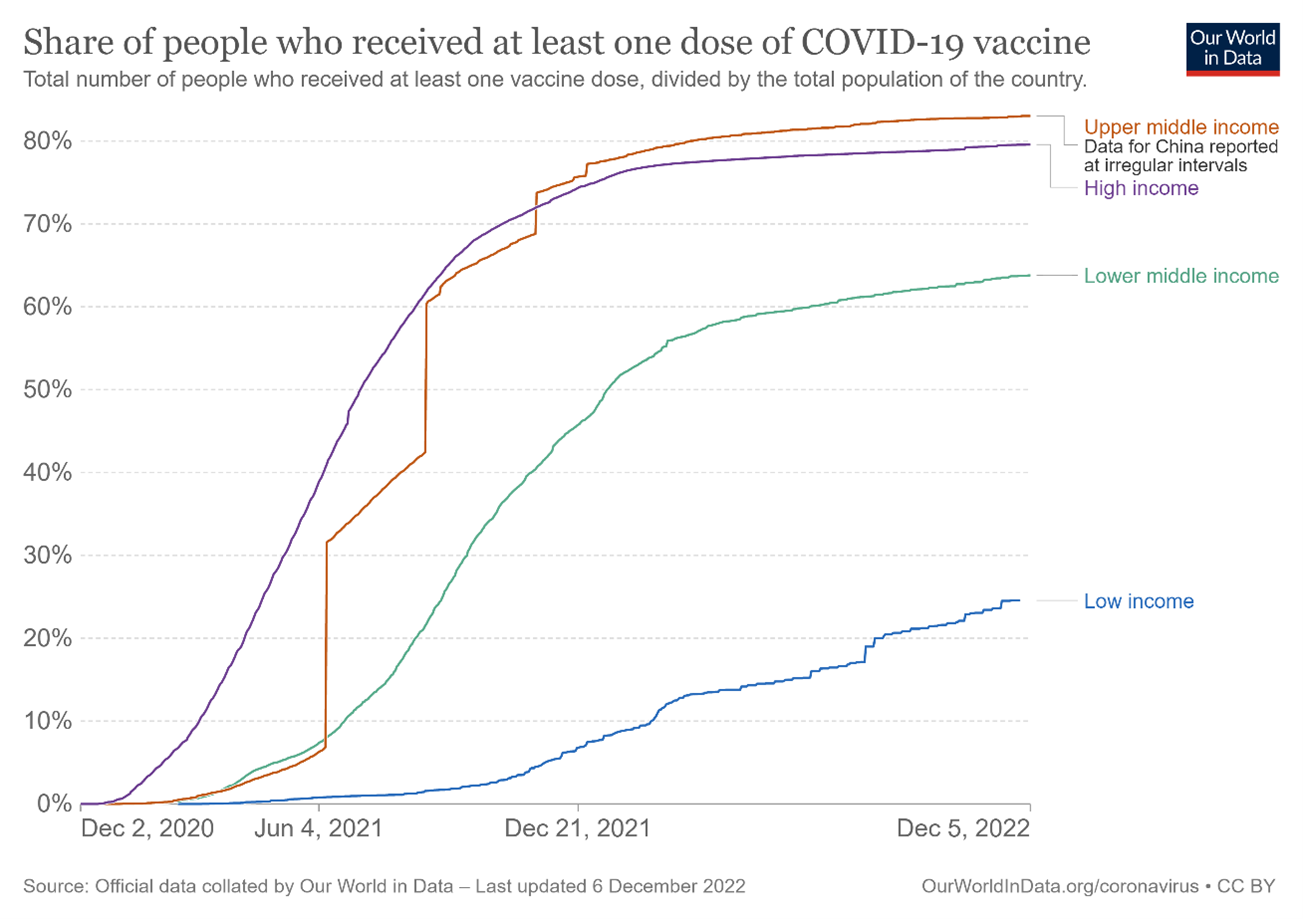
Fig. 1 – Global vaccination rates per country as of 5 December 2022
In Figure 2, we illustrate how the historical racialized processes of slavery and colonialism have driven modes of capital accumulation causing global power asymmetries that contribute to vaccine inequity. The ultimate objective of racial capitalism is to generate excessive surplus wealth for countries in the Global North, while simultaneously impoverishing countries in the Global South. This in turn, sustains the social and economic forms of inequality that are produced through reliance on modes of accumulation grounded in historically racialized practices. There are also “enablers” of racial capitalism, which are subdivided into are the institutional settings, international legal frameworks, transnational corporations, and charitable initiatives. This paper argues that all these categories contribute to, and thus enable racial capitalism within the context of COVID-19 vaccine allocation globally. The dotted lines on the flowchart reflect the complex ways in which the components set out in this paper interact. Global health is an institutional setting with colonial roots, but which has also been augmented by international legal frameworks such as the TRIPS Agreement for patent protection to guard the economic interests of large transnational pharmaceutical corporations which are largely based in the Global North. Attempts to ameliorate the situation of vaccine inequity through charitable initiatives such as COVAX and C-TAP in the wake of the current COVID-19 crisis have merely served to reproduce the colonial logic of Global South dependency on the Global North.
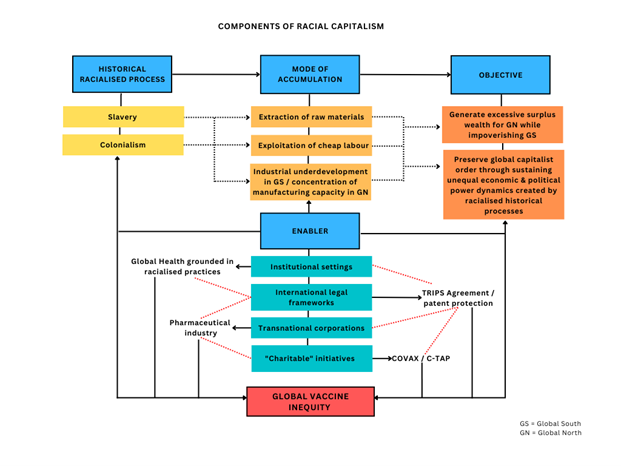
Fig. 2 – Racial Capitalism and Global Vaccine Inequity Flowchart
Unrealized aspirations: COVAX and C-TAP
COVAX
COVAX was the world’s most prominent effort to ensure equitable access to COVID-19 vaccines. Launched as part of the Access to COVID-19 Tools Accelerator in June 2020, COVAX aimed to serve as a vaccine buyers’ and distribution club for countries around the world. It also intended to support the pharmaceutical industry in speeding up COVID-19 vaccine development, vaccine manufacturing, and to ensure countries received adequate doses to vaccinate their populations, regardless of that country’s ability to pay for such vaccines. This multilateral charity model derived from the contention by Global North countries that many countries in the Global South were unable to manufacture their own vaccines[28]. As such, the scheme served to invisibilize structural racism and to deflect attention away from remedying the fractured system of global health through opting for more sustainable solutions to global vaccine inequity[29].
The inadequacies of the COVAX initiative have been grounded in three main critiques. The first is around the failure to produce and distribute vaccines because of the creation of a two-track system that allowed the wealthiest countries to acquire excessive vaccine doses through advanced market commitments. The second relates to a lack of transparency around the pricing of vaccines that led to many countries in the Global South paying more than double for the same product than the European Union and USA did[30]. The third and most critical to the argument in this paper speaks to a charity discourse, which perpetuates the false narrative that LMICs must depend on high-income countries (HICs) for access to essential medicines. This charity discourse emanates from a colonial logic that saw the restructuring of economies of colonized territories by colonizers so to create a relationship of economic dependence, and has profound implications for racial justice and inequality[31]. At the heart of the COVAX model was a privileging of risk from countries of the Global North which housed large pharmaceutical corporations. The outcome was the distortion of vaccines from a public good to a quasi-privatized good that benefitted Global North-based pharmaceutical corporations which through state aid.
C-TAP
C-TAP is a platform that was set up by WHO, the Government of Costa Rica and other partners in May 2020 to scale-up global access to COVID-19 health technologies. It aimed to facilitate the sharing of intellectual property, knowledge and data by health technology developers with manufacturers through the use of voluntary non-exclusive licenses and royalties[32]. However, the refusal of the pharmaceutical industry to engage with the voluntary initiative, instead preferring to protect their short-term exorbitant profits over realizing global public health aims (despite the fact that vaccine development and clinical trials for COVID-19 vaccines were largely publicly funded)[33], meant that the high expectations for C-TAP have not been realized[34].
These two schemes illustrate a wider issue around the lack of manufacturing capacity that has its origins in pre-colonial times[35]. Colonizers, who were focused on building corporations in their home countries in the Global North adopted an extractivist and exploitative model which saw raw materials being exported for sale on international markets[36]. Such an approach has meant that many formerly colonized nations in the Global South were never given a viable opportunity to industrialize and economically flourish on their own terms without external interference. There is a direct connection between the historical racialized processes of slavery and colonialism and the modes of capital accumulation this paper identifies in Fig. 2, and the current lack of capacity in many LMICs in the Global South to manufacture vaccines and other essential medicines.
Why the future of vaccine manufacturing in a post-COVID-19 world remains uncertain
On 21 June 2021, WHO announced that the objective of the mRNA technology transfer hub would be to build capacity in LMICs to produce mRNA vaccines[37]. The hub is located at Afrigen, Cape Town, South Africa, and is working with a network of technology recipients (called “spokes”) in LMICs to train them and transfer technology for a reverse-engineered version of Moderna’s mRNA based COVID-19 vaccine. Fifteen countries in Africa, Latin America, India and Eastern Europe have already been chosen as spokes, and IP from new technologies will be available freely[38]. While filled with promise, the reality is that spokes will not be able to distribute doses of the new vaccine until its clinical trials have been completed, which may not be until the end of 2023. Thailand and Vietnam’s ability to produce COVID-19 vaccines was made possible, at least in part, because of the legacy of the WHO Global Pandemic Influenza Action Plan, a technology transfer program run by the WHO in 2006[39]. This highlights the potential of the new WHO-backed initiative to scale up the development of mRNA technology in South Africa.
However, we identify four fundamental problems with the model of new technology hubs, and how these perpetuate a colonial extractivist capitalist model. The first is the lack of progress with further provisions around diagnostics and therapeutics in TRIPS waiver agreements, which would help with the sustainability of these new factories but are also critical to enable progress in future crises. C-TAP has been ineffectual because no legal framework exists to ensure scientific cooperation in the sharing of technology, knowledge and data when new essential medicines are developed[40]. Thus, without changes in global health law to ensure that corporations in the Global North have legally binding obligations to share scientific knowledge, any focus on relying on existing hubs to reverse engineer vaccines would always be a much slower and less feasible alternative to manufacturing vaccines in a global health crisis.
Second, there is nothing to protect these new and fledgling industries from competition from existing pharmaceutical corporations in the same jurisdictions. There is a focus extensively on TRIPS when pharmaceuticals are considered, but the GATT rules also opened markets to competition. Thus, many countries in the Global South have expanded their markets for public goods with disastrous consequences. Capitalist corporations have engaged in monopolies to kill the competition in various industries, so there is no reason to believe that the pharmaceutical industry would be any different. Here, for instance, there are no guarantees that countries in the Global North will be obliged to recognize the legitimacy of vaccines manufactured and produced in the Global South without a global system to regulate them, as was seen in the COVID-19 pandemic[41].
Third, there is a lack of clarification about the profit-making status of new vaccine manufacturing facilities that will produce pharmaceuticals in the Global South. For instance, the Serum Institute in India grossly increased its prices at the height of the second wave of COVID-19 in India which made it more expensive for the national government to procure those domestically manufactured vaccines[42].
Lastly, this model remains embedded in a broader charity discourse with colonial roots that necessitates Global South dependency on the Global North[43]. It is supported by donations (and financed by some wealthy nations and philanthropists) and does not create legal mechanisms to modify the system to one that is based on public goods from manufacturers being available for free within the context of a health crisis. Fundamentally, there is still a reliance on thinking about manufacturing in the Global South without fundamentally repairing the system through reparative justice.
A brave new world: Reparative justice for redressing racial-capitalist harms
Applying the lens of racial capitalism emphasizes the correlations between historical racialized processes and present distributions of privilege and abjection, creating pathways for restorative justice and reparations[44]. Reparative justice allows us to discern responsibility for violations over national frontiers of both the state and the private sector[45]. It focuses on transforming relationships “in which there has been chronic disregard and repetitive abuse”[46], such as in cases where victims of injustice have perpetually suffered from structural violence predicated on historical racialized practices in the quest to accumulate excessive surpluses of capital. Currently there are attempts to reform global health law through either the implementation of a pandemic treaty or making further revisions to the International Health Regulations (IHR). We make two major propositions for a global reparative justice agenda for vaccine equity.
The first proposition relates to reforming the international IP system. The TRIPS Agreement contains rules that constrain the wide manufacture of vaccines and other essential medicines during health crises and sustains unequal economic and geopolitical dynamics created by historically racialized processes. Attempts to implement new treaties must be revolutionary in defining pandemics as a state of exception in which patent rules under international trade law cannot be allowed to stand.
The second proposition is around ensuring global commitment for an ambitious long-term financing agenda. Such commitment would mean supporting the manufacture and purchase of vaccines in LMICs based in the Global South, so that these new industries can not only survive but also be competitive in global markets[47]. This long-term financing would cement vaccines as a global public good, in line with the obligations of states and corporations to protect human rights, including the right to health, in order to ensure that in times of crisis vaccines are manufactured with a focus on providing for the global population as opposed to facilitating the unjust enrichment of Global North-based pharmaceutical corporations.
This paper calls for changing both law and funding structures as mechanism of reparative justice. While on the one hand, law plays a role in sustaining racial-capitalist harms, it can also be used as a tool for facilitating reparative justice[48]. As the enforcement and jurisdictional limitations of the IHR became clear during the COVID-19 pandemic[49], revisions of the IHR and a pandemic treaty offer the world a more robust way of embedding a global reparative justice agenda for vaccine equity in global health law to guard against nationalistic practices which undermine equal access to essential medicines for all.
Conclusion
Racial capitalism, as a framework to analyze the mutually constitutive nature of racialization and capitalist exploitation, enables a more thorough understanding of the root causes of global vaccine inequity. Tracing the ways in which the historical racialized processes of slavery and colonialism have driven modes of capital accumulation illuminate how those processes have shaped asymmetrical power relations and led to unequal divisions of resources globally. This in turn has had a calamitous and disproportionate impact on access to essential medicines for Global South populations. While the development of global health law has colonial underpinnings, this paper has contends that it is also playing an active role in sustaining the dynamics created by those legacies. An analysis of the contemporary solutions to vaccine inequity during the COVID-19 pandemic, namely COVAX and C-TAP, using the framework of racial capitalism reveals why these “charitable” initiatives failed to accomplish their aims. They could not succeed because they were imbued with racially-capitalist logics which are completely incompatible with the concept of equity and human rights. Conversely, initiatives yielding enormous promise, such as new manufacturing hubs situated in LMICs, will need to pay attention to the underlying racialist-capitalist nature of the current arrangements behind these solutions. Without changing tack and relinquishing the colonially constructed charity discourse that governs initiatives backed by Global North actors, solutions to vaccine inequity may succeed only in exacerbating inequalities. The prospect of reparative justice for redressing racial-capitalist harms, however, offers a way to reimagine a world where equitable access to essential medicines such as vaccines during a health crisis is possible. Rather than doing what has always been done—that is, accepting a broken system that manufactures inequality—reforming the international IP system and ensuring global commitment for new long-term financing arrangements to support the manufacturing in and the purchase of vaccines from LMICs are two important reparative justice measures for manufacturing a more sustainable and equitable future for the global population, of which we are all a part.
References
* Sharifah Sekalala, PhD, LLMB, LLBM, is Professor of Global Health Law in the School of Law at the University of Warwick, Coventry, United Kingdom.
*Belinda Rawson BA, LLB, is an Associate Tutor and Research Assistant in the School of Law at the University of Warwick, Coventry, United Kingdom.
The article draws on the ILJ-JILP Symposium on Inter-Pandemic Regulation, and we would like to thank the participants for their insightful questions and suggestions as well as Dr. Amanda Wilson, Dr. Colin Foster and Prof. James Harrison who provided oral and written feedback on the ideas expressed in this piece. Any errors are our own. We would also like to thank the Connaught Foundation for funding for this work.
[1] U.N. GENERAL ASSEMBLY, High-level meeting of the General Assembly to commemorate the twentieth anniversary of the adoption of the Durban Declaration and Programme of Action (A/HRC/42/45, at 2) (Sep. 22, 2021), https://documents-dds-ny.un.org/doc/UNDOC/GEN/N21/260/73/pdf/N2126073.pdf?OpenElement.
[2] U.N. GENERAL ASSEMBLY, supra note 1, at 3.
[3] See Harold Wolpe, Capitalism and cheap labour-power in South Africa: from segregation to apartheid, ECON SOC, 1(4), 425–456 (1972); Martin Legassick & David Hemson, Foreign Investment and the Reproduction of Racial Capitalism in South Africa, ANTI-APARTHEID MOVEMENT, UTC LIBRARIES SPECIAL COLLECTION BC1150 A2(2) (1976), www.sahistory.org.za/archive/foreign-investment-and-reproduction-racial-capitalism-south-africa-martin-legassick-and; NO SIZWE (PSEUD.), NEVILLE ALEXANDER, ONE AZANIA, ONE NATION: THE NATIONAL QUESTION IN SOUTH AFRICA (1979).
[4] CEDRIC J. ROBINSON, BLACK MARXISM: THE MAKING OF THE BLACK RADICAL TRADITION (The University of North Carolina Press 2000) (1983).
[5] GARGI BHATTACHARYYA, RETHINKING RACIAL CAPITALISM: QUESTIONS OF REPRODUCTION AND SURVIVAL, at 38 & 77 (2018).
[6] Carmen Gonzalez & Athena Mutua, Mapping Racial Capitalism: Implications for Law, J POLIT ECON, 2(2), 127–201 (2022).
[7] ANDY CLARNO, NEOLIBERAL APARTHEID: PALESTINE/ISRAEL AND SOUTH AFRICA AFTER 1994, 1-23 (2017).
[8] Carmen G. Gonzalez, Racial capitalism, climate justice, and climate displacement, OÑATI SOCIO-LEGAL SERIES, 11(1), 108–147 (2021).
[9] Christopher Gevers, Refiguring Slavery Through International Law: The 1926 Slavery Convention, the ‘Native Labor Code’ and Racial Capitalism, J. INT. ECON. LAW, 25(2), 312–333 (2022).
[10] Charisse Burden-Stelly, Modern U.S. Racial Capitalism: Some Theoretical Insights, MONTHLY REVIEW, 72(3), 8–20 (2020); Ali Mir & Saadia Toor, Racial capitalism and student debt in the U.S., ORGANIZATION, 00(0), 1–12 (2021); Hossein Ayazi, Land reform, race reform: Interwar anticommunism and U.S. racial capitalism, ENVIRON. PLAN. D: SOC. SPACE, 40(5), 900–922 (2022).
[11] Whitney N. Laster Pirtle, Racial Capitalism: A Fundamental Cause of Novel Coronavirus (COVID-19) Pandemic Inequities in the United States, HEALTH EDUC BEHAV, 47(4), 504–508 (2020).
[12] Zophia Edwards, Racial Capitalism and COVID-19: How racial capitalism, and not just capitalism, shapes exploitation and solidarities, THE JUS SEMPER GLOBAL ALLIANCE (2021), https://monthlyreview.org/2021/03/01/racial-capitalism-and-covid-19/.
[13] Rieke van der Graff, et al., Vaccine equity: Past, present, and future, CELL REP, 3(3), 1–4 (2022).
[14] RANDALL M. PACKARD, Post-Colonial Medicine, in MEDICINE IN THE TWENTIETH CENTURY 98 (Roger Cooter & John Pickstone, eds., 2000).
[15] PACKARD, supra note 14, at 99.
[16] PACKARD, supra note 14, at 97–112; Delivette Castor & Luisa N. Borrell, The cognitive dissonance discourse of evolving terminology from colonial medicine to global health and inaction towards equity – A Preventive Medicine Golden Jubilee Article, PREV. MED, 163(107227) 1–4 (2022); Jin Un Kim, et al., A time for new north–south relationships in global health, INT. J. GEN. MED., 10, at 402 (2017).
[17] NTINA TZOUVALA, CAPITALISM AS CIVILISATION: A HISTORY OF INTERNATIONAL LAW (2020).
[18] Gonzalez & Mutua, supra note 6, at 137.
[19] Daniella Coleman, Digital Colonialism: The 21st Century Scramble for Africa through the Extraction and Control of User Data and the Limitations of Data Protection Laws, MICH. J. RACE & L., 24(2), at 421 (2019).
[20] Samantha Vanderslott & Tatjana Marks, Travel restrictions as a disease control measure: Lessons from yellow fever, GLOB. PUBLIC HEALTH, 16(3), 319–484 (2021).
[21] Sharifah Sekalala & Belinda Rawson, Navigating the Paradoxes of Selective COVID-19 Border Closures, BORDER CRIMINOLOGIES (Jul. 8, 2020), www.law.ox.ac.uk/research-subject-groups/centre-criminology/centreborder-criminologies/blog/2020/07/navigating; Sarah Hodges, et al. When suspicion replaces evidence in public health, LANCET, 398(10311), 1565–1566 (2021).
[22] JOHN LOCKE, TWO TREATISES OF GOVERNMENT 285–302 (Cambridge University Press 1988) (1689); Barbara Arneil, Trade, Plantations, and Property: John Locke and the Economic Defense of Colonialism, JHI, 55(4), 591–609 (1994).
[23] AMAKA VANNI, Lessons from COVID-19 for Medicines Access, in INTELLECTUAL PROPERTY LAW AND ACCESS TO MEDICINES: TRIPS AGREEMENT, HEALTH, AND PHARMACEUTICALS, 485–496 (Srividhya Ragavan & Amaka Vanni, eds., 2021).
[24] Ellen R. Shaffer, et al., Global Trade and Public Health, AM. J. PUBLIC HEALTH, 95(1), 23–34 (2005); LISA FORMAN, Trading health for profit: bilateral and regional free trade agreements affecting domestic property rules on pharmaceuticals, in THE POWER OF PILLS: SOCIAL, ETHICAL AND LEGAL ISSUES IN DRUG DEVELOPMENT, MARKETING, AND PRICING, 190–199 (Jillian Clare Cohen, et al., eds., 2006).
[25] Sharifah Sekalala & Belinda Rawson, The Role of Civil Society in Mobilizing Human Rights Struggles for Essential Medicines: A Critique from HIV/AIDS to COVID-19, HEALTH HUM. RIGHTS, 24(2), 177–189 (2022).
[26] SRIVIDHYA RAGAVAN & AMAKA VANNI, INTELLECTUAL PROPERTY LAW AND ACCESS TO MEDICINES: TRIPS AGREEMENT, HEALTH, AND PHARMACEUTICALS, 1–21 (2021); VANNI, supra note 24, at 485–496.
[27] Our World in Data, Coronavirus (COVID-19) Vaccinations), OUR WORLD IN DATA, (Dec. 5, 2022), https://ourworldindata.org/grapher/share-people-vaccinated-covid?country=High+income~Upper+middle+income~Lower+middle+income~Low+income.
[28] Elisabeth Mahase, Covid-19: Public vaccine funding needs “strings attached” for equitable access, say campaigners, BMJ, 376:o565, 1 (2022).
[29] Sophie Harman, et al., Global vaccine equity demands reparative justice — not charity, BMJ GLOB. HEALTH, 6:e00650, 1–4 (2021).
[30] Katrina Perehudoff, European governments should align medicines pricing practices with global transparency norms and legal principles, LANCET REG, 16(100375), 1–2 (2022).
[31] Tendayi Achiume, Global extractivism and racial equality: Report of the Special Rapporteur on contemporary forms of racism, racial discrimination, xenophobia and related intolerance, U.N. HUMAN RIGHTS COUNCIL (May 14, 2019), https://digitallibrary.un.org/record/3823039?ln=en.
[32] WHO, WHO COVID-19 Technology Access Pool, WHO (2020), www.who.int/initiatives/covid-19-technology-access-pool.
[33] Hussain S. Lalani, et al., US Taxpayers Heavily Funded the Discovery of COVID‐19 Vaccines, CLIN. PHARM. THERAP, 111(3), 542–544 (2022); Aris Angelis, et al., Funding Sources of Therapeutic and Vaccine Clinical Trials for COVID-19 vs Non–COVID-19 Indications, 2020-2021, JAMA NETW. OPEN, 5(8), e2226892 (Aug. 16, 2022).
[34] Health Action International, C-TAP has not (yet) lived up to high expectations, HAI, (May 28, 2021), https://haiweb.org/c-tap-has-not-yet-lived-up-to-high-expectations/; Ellen ‘t Hoen, et al., Scaling-up Vaccine Production Capacity: Legal Challenges and Recommendations. Background paper 6, (Commissioned by The Independent Panel for Pandemic Preparedness and Response) (2021), https://theindependentpanel.org/wp-content/uploads/2021/05/Background-paper-6-Scaling-up-vaccinationlegal-aspects.pdf.
[35] KWAME NKURUMAH, NEO-COLONIALISM: THE LAST STAGE OF IMPERIALISM (1965).
[36] See Harold Wolpe, Class, Race and the Occupational Structure in South Africa (Paper delivered to the World Sociology Congress, September 1970) (1971), https://sas-space.sas.ac.uk/3646/; Michael Fakhri, Markets, Sovereignty, and Racialization, J. INT. ECON. LAW, 25(2), 242–258 (2022); Kojo Koram, The Legalization of Cannabis and the Question of Reparations, J. INT. ECON. LAW, 25(2), 294–311 (2022).
[37] WHO, WHO supporting South African consortium to establish first COVID mRNA vaccine technology transfer hub, WHO (Jun. 21, 2021), www.who.int/news/item/21-06-2021-who-supporting-south-african-consortium-to-establish-first-covid-mrna-vaccine-technology-transfer-hub.
[38] Medicines Patent Pool, WHO and MPP announce names of 15 manufactures to receive training from mRNA technology transfer hub, MPP (Apr. 19, 2022), https://medicinespatentpool.org/news-publications-post/who-and-mpp-announce-names-of-15-manufactures-to-receive-training-from-mrna-technology-transfer-hub.
[39] Aisling Irwin, How COVID spurred Africa to plot a vaccines revolution, NATURE (Apr. 21, 2021), www.nature.com/articles/d41586-021-01048-1; Elizabeth F. Peacocke, et al., Global access to COVID-19 vaccines: a scoping review of factors that may influence equitable access for low and middle-income countries, BMJ OPEN, 11:e049505, 1–11 (2021).
[40] VANNI, supra note 24, at 485–496.
[41] CTV News, South Africa rejects 2 million J&J vaccines due to FDA decision, CTV NEWS (Jun. 14, 2021), www.ctvnews.ca/health/coronavirus/south-africa-rejects-2-million-j-j-vaccines-due-to-fda-decision-1.5469505.
[42] Aftab Ahmed, India to fund capacity boost at Serum Institute, Bharat Biotech as vaccines run short, REUTERS (Apr. 19, 2021), www.reuters.com/world/india/india-fund-capacity-boost-serum-institute-vaccines-run-short-source-2021-04-19/.
[43] Harman, et al., supra note 30.
[44] Walter Johnson, To Remake the World: Slavery, Racial Capitalism, and Justice, BOSTON REVIEW (Feb. 20, 2018), www.bostonreview.net/forum/walter-johnson-to-remake-the-world/.
[45] JOHN HARRINGTON & MARIA STUTTAFORD, GLOBAL HEALTH AND HUMAN RIGHTS: LEGAL AND PHILOSOPHICAL PERSPECTIVES 6 (2010).
[46] MARGARET URBAN WALKER, WHAT IS REPARATIVE JUSTICE? 25 (2010).
[47] Irwin, supra note 40; Lowri Davies, Compulsory licensing: An effective tool for securing access to Covid-19 vaccines for developing states?, LEGAL STUDIES, 1–18 (2022).
[48] ANNETTE BAIER, REFLECTIONS ON HOW WE LIVE, 1–15 (2010).
[49] Elliot Hannon, et al., Why we still need a pandemic treaty, LANCET GLOB. HEALTH, 10(9), E1232–E1233 (2022).